21,99 €
Mehr erfahren.
- Herausgeber: John Wiley & Sons
- Kategorie: Bildung
- Sprache: Englisch
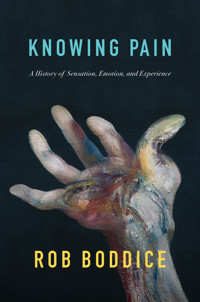
Pain, while known to almost everyone, is not universal. The evidence of our own pain, and our own experience, does not provide us with automatic insight into the pains of others, past or present. No matter how self-evident and ubiquitous the sting of a paper cut or the desolation of heartbreak might seem, pain is situated and historically specific. In a work that is sometimes personal, always political, Rob Boddice reveals a history of pain that juggles many disciplinary approaches and disparate languages to tackle the thorniest challenges in pain research. He explores the shifting meaning-making processes that produce painful experiences, expanding the world of pain to take seriously the relationship between pain's physicality and social and emotional suffering. Ranging from antiquity to the present and taking in pain knowledge and pain experiences from around the world, his tale encompasses not only injury, but also grief, exclusion, chronic pain, and trauma, and reveals how knowledge claims about pain occupy what pain is like. Innovative and compassionate in equal measure, Knowing Pain puts forward an original pain agenda that is essential reading for those interested in the history of emotions, senses, and experience, for medical researchers and practitioners, and for anyone who has known pain.
Sie lesen das E-Book in den Legimi-Apps auf:
Seitenzahl: 514
Veröffentlichungsjahr: 2023
Ähnliche







Table of Contents
Cover
Dedication
Title Page
Copyright Page
Figures
Acknowledgements
Prologue
Notes
Introduction: Disrupting a Definition
Definitions: A Contemporary Overview
Sense and Emotion
Notes
1
Scripting
: The Politics of Knowledge
From Greek Pain to Arabic Pain
From Arabic Pain to Renaissance Pain
Eastern Schools
Modern Pain Pathways
Notes
2
Experiencing
: Objectivity versus Subjectivity
Pain by Numbers
The Figural Face
Feeling the Flow
Trauma
Achilles: Grief Personified
Notes
3
Worlding
: Expressing and Managing
Our Lady of the Tumours
Going Under
Of Use and Uselessness
Worlding through Art
Notes
4
Suffering
: Chronicity and Pain Syndromes
Making Chronic Pain Knowledge
The Subjectivity Gap: MPQ
Memory and Re-experienced Pain
Outing Pain
Fronto’s Crip Time?
Notes
5
Commiserating
: Sensing, Feeling, and Witnessing the Other in Pain
The Animal in Pain?
According to the Human Thing
Sympathy in the Sick-Room?
Empathy
Notes
6
Contextualizing
: Pleasure and Punishment
Torture Worlds
Discipline and Punish
Agony and Ecstasy
Pushing the Pain Barrier
Notes
7
Embodying
: Nocebo/Placebo
Accounting for Placebo in the Past
The Current Outlook on Placebo
The Attitude of Placebo Scientists to the Past
Epistles from Madeira
Nocebo Effects: From COVID-19 to Hysteria
Voodoo? Nocebo and the Enduring Puzzle of the Hex
Routes Forward
Notes
Conclusion: The Mutable Patient
Notes
Epilogue
Notes
Bibliography
Index
End User License Agreement
List of Illustrations
Chapter 2
Figure 1.
Charles Le Brun,
Extrême Douleur corporelle
(1702). (Metropolitan ...
Figure 2.
Charles Le Brun,
Douleur Egüe
(1702). (Rijksmuseum.)
Figure 3.
Charles Le Brun,
Douleur aigue de corps et d’Ésprit
(1702)....
Figure 4.
Charles Le Brun,
Mouvement de douleur
(1702). (Metropolitan Museum of Art...
Figure 5.
Charles Bell,
Pain of the sick, and in some degree subdued by continual suffering
...
Figure 6.
Charles Bell,
Utmost extremity of pain
(1806). (Wellcome Collection.)
Figure 7.
Charles Bell,
True Opisthotonos
(1824). (Wellcome Collection.)
Figure 8.
Guillaume-Benjamin-Amand Duchenne de Boulogne,
Pain and Despair
(1854–...
Figure 9.
A sequence of facial changes showing the emergence of the four principal facial ...
Figure 10.
Wong–Baker Pain Faces Scale. (Donna Lee Wong and Connie Morain Baker, ‘...
Figure 11.
Pain avatar. (Eleonora Meister et al., ‘Decoding of facial expressions of...
Figure 12.
Thetis presenting Achilles with his new armour, c.460
bce
, Attic ...
Chapter 3
Figure 13.
Luca Longhi,
St Agatha
(sixteenth century), Basilica de Santa Maria Maggi...
Figure 14.
Edvard Munch, study for
Fortvilelse
(1892). (Munch Museum.)
Figure 15.
Mladen Stilinović’s
Dictionary – Pain
(2000–...
Figure 16.
Louise Bourgeois,
The Arch of Hysteria
(1993). (© The Easton Found...
Chapter 5
Figure 17.
Clemente Susini,
Venerina
(1782), Palazzo Poggi, Bologna. (Photograph by ...
Chapter 6
Figure 18.
Scold’s bridle (sixteenth–eighteenth century), Science Museum, Lon...
Guide
Cover
Table of Contents
Begin Reading
Pages
ii
iii
iv
vi
vii
viii
ix
x
xi
xii
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
246
247
248
249
250
251
252
253
254
255
256
Dedication
For Tony Morris
KNOWING PAIN
A History of Sensation, Emotion, and Experience
Rob Boddice
polity
Copyright Page
Copyright © Rob Boddice 2023
The right of Rob Boddice to be identified as Author of this Work has been asserted in accordance with the UK Copyright, Designs and Patents Act 1988.
First published in 2023 by Polity Press
Polity Press
65 Bridge Street
Cambridge CB2 1UR, UK
Polity Press
111 River Street
Hoboken, NJ 07030, USA
All rights reserved. Except for the quotation of short passages for the purpose of criticism and review, no part of this publication may be reproduced, stored in a retrieval system or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publisher.
ISBN-13: 978-1-5095-5054-8
A catalogue record for this book is available from the British Library.
Library of Congress Control Number: 2022946076
by Fakenham Prepress Solutions, Fakenham, Norfolk NR21 8NL
The publisher has used its best endeavours to ensure that the URLs for external websites referred to in this book are correct and active at the time of going to press. However, the publisher has no responsibility for the websites and can make no guarantee that a site will remain live or that the content is or will remain appropriate.
Every effort has been made to trace all copyright holders, but if any have been overlooked the publisher will be pleased to include any necessary credits in any subsequent reprint or edition.
For further information on Polity, visit our website: politybooks.com
Figures
1 Charles Le Brun, Extrême Douleur corporelle (1702)
2 Charles Le Brun, Douleur Egüe (1702)
3 Charles Le Brun, Douleur aigue de corps et d’Ésprit (1702)
4 Charles Le Brun, Mouvement de douleur (1702)
5 Charles Bell, Pain of the sick, and in some degree subdued by continual suffering (1806)
6 Charles Bell, Utmost extremity of pain (1806)
7 Charles Bell, True Opisthotonos (1824)
8 Guillaume-Benjamin-Amand Duchenne de Boulogne, Pain and Despair (1854–6)
9 A sequence of facial changes showing the emergence of the four principal facial actions
10 Wong–Baker Pain Faces Scale
11 Pain avatar
12 Thetis presenting Achilles with his new armour, c.460 bce, Attic red-figure volute-krater, Louvre, Paris
13 Luca Longhi, St Agatha (sixteenth century), Basilica de Santa Maria Maggiore, Ravenna
14 Edvard Munch, study for Fortvilelse (1892)
15 Mladen Stilinović, Dictionary – Pain (2000–3)
16 Louise Bourgeois, The Arch of Hysteria (1993)
17 Clemente Susini, Venerina (1782), Palazzo Poggi, Bologna
18 Scold’s bridle (sixteenth–eighteenth century), Science Museum, London
Acknowledgements
I began researching the history of pain in 2003. Despite the long gestation, the book came together quickly: an unexpected and positive turn after the conclusion of an unfortunate affair. For this I heap great praise on Pascal Porcheron at Polity and my stalwart agent Tony Morris for attaching rocket boosters to the idea for Knowing Pain. I am indebted to Joanna Bourke, Ian Miller, and Javier Moscoso for championing this book. It would not have been possible without the support of colleagues and family. Thanks to Pertti Haapala, Pirjo Markkola, Raisa Toivo, Ville Kivimäki, Bianca Frohne, David Turner, and Daniel Goldberg. Parts of the manuscript were shared at the colloque de l’Institut Éthique Histoire Humanités in the Faculté de Médecine, Université de Genève, thanks to Dolores Martín Moruno; at the ‘Emotions, History and the Body’ seminar at the University of York, thanks to Fay Bound Alberti; at the conference ‘Establishing Empathy: Education, Emotions and Society in the Nineteenth and Twentieth Centuries’ at Hamburg University, thanks to Esther Möller, Sylvia Kesper-Biermann, and Katharina Stornig; and at the cross-faculty seminar series ‘Animal and Human Emotions’ at the University of Newcastle, thanks to Lutz Sauerteig and Carmen Hubbard. Marie van Haaster materially helped with the placebo chapter. Sara Honarmand Ebrahimi was immeasurably helpful with Arabic and Farsi and, with Anneleen Arnout, in tracking down difficult-to-find texts. The book was written between Montreal and Tampere. It would not have been possible without Stephanie and Sébastien always close by. The context of disease, war, fear, and suffering would be paralysing without them.
Prologue
I am looking at my own brain stem. It is 1995.
Gazing at myself, sliced in sections, layer upon layer, I see myself but do not recognize these images as me. Stacked underneath the brain stem are the cervical vertebrae, each sandwiching a vertebral disc: sectional images, like postcards from the interior. Four or five into the sequence, the surgeon says, ‘Ah-ha.’ The disc between C4 and C5 is herniated, the split in its surface visible on the magnetic resonance image (MRI). This is my pain. The jellyish nucleus of the disc has been poking out of the annulus, touching off nerves that feel like hot needles, sending my neck and shoulders into paralysing spasms. By the point of discovery, this has already been going on for months. I have been in agony, doubled over like an old man, unable to turn my head left or right, sometimes feeling unable to move at all. It’s taken some flexing to get a diagnosis. I am 17 years old.
My recovery, if I can call it that, is now in its 28th year.
I am recounting what I know about my own pain, what it is and what I remember of it, so that I can document its situatedness and its particularities, and so that I can dismiss it. It is pertinent not as an exemplar of chronic neck and shoulder pain, but as a particular experience of pain. I can show how and why this pain was meaningful, for the purpose of showing that it affords me no direct insight into the pain of others. If the evidence of my own experience is any kind of guide, then it is a guide only to the importance of context, structure, script, and culture in the meaning-making processes of subjective pain. A herniated disc and the genetic weakness that makes it happen again and again can be explained. Its associated effects and debilitations can be loosely predicted. But the quality and meaning of the pain depend upon all manner of ingredients that are not intrinsic to the spine. A pain in the neck is not simply a pain in the neck. Working out all these ingredients will involve a trip a bit higher up, to the brain, and a trip out, to the post-Thatcherite desolation of working-class South Derbyshire in the early 1990s, to the fine-grained distinctions of social class, and to the intransigence of an NHS general practitioner to the causes, consequences, treatment, and experience of chronic pain.1 Should you herniate a disc, you would have to undertake a similar journey upwards and outwards.
Others had witnessed my decline. My posture slumped. Sitting at a desk became intolerable. Iron claws would grip my shoulders, above the collar-bone, and the thumbs of those claws would penetrate under the shoulder-blades. I was held in a vice with spikes.
It took courage to go to a doctor. Visiting came with guilt. Am I wasting his time? Am I imagining all of this? What if I don’t feel it on the day? Will he think I’m a fraud? Shouldn’t I be tougher than this? My self-examination was, in the event, in excess of the examination I received at the hands of the doctor. Quickly dismissed with a prescription for ibuprofen, without physical examination, I went on my way feeling that I had not been heard at all. I went back to the same doctor twice more. I was never examined, but simply prescribed stronger doses of ibuprofen. After the third visit, and many months, the dose was upped to 800 mg pink horse pills and there seemed to be no end in sight. The pills did nothing except cause alarm.
At this point, my parents intervened. They were self-employed, small-business owners. For a short period in our lives, we had private health insurance – BUPA – which was available as a means of avoiding the NHS queue for those willing to pay. None of us had ever used it. In a public health system, it was deeply divisive and hard to square with the principle of a National Health Service. I was not engaged in any of this. All I knew was that the doctor was not doing anything either to find the cause of my problem or to actively fix it.
A new appointment was made, with a different doctor at the same practice. The story, which by this point was a story of being in agony and being ignored, was recounted. My dad mentioned that we were in BUPA. At a stroke, the game changed. We were asked whom we would like to see. My dad mentioned the name of a surgeon he knew – not personally, but because he was the go-to guy for Derby County Football Club – and in no time at all I became his private patient, in his rooms in part of his own house. An MRI scan was quickly scheduled in a private hospital (it had carpets and did not smell of disinfectant; it felt more like a hotel) with a diagnosis following on directly. A course of physiotherapy followed, without further waiting. In school, since I’d had time off, my form teacher asked me about it in front of the whole class, and I explained in the context of my dad’s own long struggles with cervical spondylosis how, as the surgeon had put it to me, ‘the emergence of dad’s problem’ in me had occurred remarkably early. Her response was a snort of derision: ‘You don’t have a cervix!’ She apologized the following day, in private, having consulted a dictionary. It did not undo the humiliation. All the time the same questions, before a variety of authorities, ran in my mind: ‘Am I allowed to have this pain, this condition? Does it help to say I’ve got this – a specific condition with some impenetrable jargon? Why isn’t the fact of being in pain enough to be believed, to be taken seriously?’
To know about the injury behind my pain was something of a relief. The prospect of recovery was an analgesic. But the process of finding it out had been an eye-opener. I could see how, without the magic wand of private healthcare, and without a parent advocate who at least knew enough to properly game the system, I might have been stuck in an infinite loop of medicated despair. I could see a route out and I could see that it was unjust.
The physiotherapist was not a listener either. She did things that hurt. In my mind, she did things designed to hurt. At one point, as she jammed her thumbs into my neck and as I yelled, it felt like a torture session. ‘Is that your pain?’ she asked, repeatedly. She had found it and was pressing it, making me own it. Of course it was my fucking pain. Who else could it have belonged to? But the cause of the pain was shifting, from a deficiency in my own body, to this person and her boring thumbs; to this room of strange equipment that put my jaw in traction; to the ultrasonic devices waved in front of me like (utterly ineffective) magic wands, and to the other people in that room, all in agonies of their own. The atmosphere that defined the room was one of pain, not of hope or recovery. Maybe, over weeks, the therapy helped. Constant attention to my posture and giving up snooker probably helped more.
The pain never went away. Or, rather, the shadow of pain never left. I know, now, that I can herniate that disc at any moment, by any innocuous activity. A long writing session at the wrong desk will do it. Standing for too long will do it. Even putting on a coat can do it. I stave it off by running (something my erstwhile physiotherapist told me never to do). About once a year, I’m out of action for a couple of weeks. I know right away when it’s happened, and I know what to expect. Every time, my mind casts back to the first time. I remember it, curse it, and try to mark the differences. It’s not the same pain now as then. Why? Because I know about it. I know its causes and its limits. I know what to do and what not to do. I know that in a pinch I can seek help from a doctor, without guilt or fear, and with the knowledge that I can request the examination and the assistance I did not receive when I first approached a doctor at the age of 17. My pain is mine. It is entangled in its own narrative that is constantly being re-written. It has been made worse or better to the extent that I am the author of that narrative. At 17, I was in control of very little and knew very little. That is no longer the case.
Notes
1
Alex Scott-Samuel et al., ‘The impact of Thatcherism on health and well-being in Britain’,
International Journal of Health Services
, 44 (2014): 53–71; Iain Crinson, ‘Putting patients first: the continuity of the consumerist discourse in health policy, from the radical right to New Labour’,
Critical Social Policy
, 55 (1998): 227–39.
IntroductionDisrupting a Definition
Everyone knows their own pain. How? This book explores the answer to this question historically, demonstrating the relationship between the pains people have known and the changing frameworks of philosophical, medical, religious, and scientific expertise that have claimed to know what pain is. It is, therefore, a contribution to current knowledge about the experience of pain, produced in a transdisciplinary space comprising perspectives from history, philosophy, anthropology, psychology, psychiatry, neuroscience, politics, art, and literary studies. Knowing Pain illuminates a history of painful experiences, a messy assemblage of many worlds of suffering, which disrupts commonplace appeals to the universality of pain. Here you will find: pain as specific, particular, mediated, and contingent; body-minds whose agonies are connected to the cultures they inhabit; brains that produce pain that makes sense only in and through the context of its experience; authorities that make and disseminate the situated concepts of pain, through which suffering is made meaningful; historical politics of the medical and moral valuation of pain; pains that count, and pains that are invalid. You will find claims that patients do not know their own pain at all and the provocation that your pain belongs to someone else’s discrimination.
This book cuts against the grain of ‘common sense’ about the pain that people think they know. It documents well-known but under-appreciated phenomena, such as the history of extraordinary and devastating injuries that, nonetheless, did not hurt; the history of overwhelming suffering unconnected to any injury at all; the unreliability of the senses as either a signal for pain or a method of measuring pain; how these mutable senses, in combination with equally contingent emotional concepts, can change the experience of pain. It shows pain as a virtue and as a pleasure, and how much of the history of human pain has fallen beyond the ken or the interest of medicine. The world of medicine nevertheless plays a big part in the story, both in terms of the production of knowledge of what pain is and how to alleviate it, and concerning its role in creating limited definitions of pain that seemingly either overlooked or failed to treat a great tide of suffering. I delve into the lived experience of pain in all its physical, emotional, social, and cultural entanglements to reveal the kinds of apparently invisible pain that millions, nonetheless, have known and shared.
Aside from collating these phenomena, this book puts forward an original pain agenda. Ranging from antiquity to the present, and taking in pain knowledge and pain experiences from around the world, I draw upon the methodology of the history of the senses, the history of emotions, and the new history of experience to weave a narrative about the mutable patient, or the situated sufferer, often alone, sometimes in a collective.1 It is predicated on critical engagement with a strain of social neuroscientific and neurohistorical research that explains how the concepts by which humans express their experiences play a central role in the production of experiences. A history of pain concepts and pain practices becomes a history of the contextualized plastic, biocultural brain-body system. Pain, an embodied, embrained, but above all meaningful experience, is in and of the world. It may be something that almost every human has known, but there is nothing in the evidence of our own experience that affords us automatic insight into the pains of others, or into the pains of the past. To that end, this book is a sustained denial of universality, and a denial of easy recognition of the other in pain. I lay bare the difficulties and the politics of knowing pain – your own, someone or something else’s – and the way that the experience of pain is mutable, historical, and unpredictable. I aim to show the connections between the construction, use, and experience of pain, understanding as a first principle that knowledge claims about pain occupy what pain is like.2
Definitions: A Contemporary Overview
Since one major purpose of this book is to historicize the experience of pain, to show that it can and does change over time, a necessary first step is to disrupt any operative definition that delimits what pain is. The formal definition of pain has focused the worlds of medicine and medical science on the kinds of pain research that are pursued and the kinds of pain that receive priority for treatment. Disrupting such definitions is essential if the varieties of pain experience, in the past and in the present, are to be recognized. In chapter 1, I will explore the historical formulations of pain, but I begin with the present and the possibilities current formal definitions afford.
The International Association for the Study of Pain (IASP) formulated a formal definition in 1979: ‘Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.’3 Critics across the disciplines found this definition inadequate, and it was finally augmented and complicated (and improved) in July 2020. A series of qualifications and clarifications have been added. They make the formal definition less pithy and supply new possibilities for the study of pain, especially in historical terms:
Pain is always a personal experience that is influenced to varying degrees by biological, psychological, and social factors.
Pain and nociception are different phenomena. Pain cannot be inferred solely from activity in sensory neurons.
Through their life experiences, individuals learn the concept of pain.
A person’s report of an experience as pain should be respected.
Although pain usually serves an adaptive role, it may have adverse effects on function and social and psychological well-being.
Verbal description is only one of several behaviors to express pain; inability to communicate does not negate the possibility that a human or a nonhuman animal experiences pain.
4
The most welcome parts of this revision are as follows. First, the notion of pain as an objective phenomenon – something that can be mechanically measured or rated – is rejected in the first clause. Pain, it confirms, is subjective. Later, I’ll explore the boundaries of this claim, showing that sometimes pain is not ‘personal’, but ‘social’, analysing the relational dynamics that colour the experience of both pain and relief. For now, it is helpful to think of pain in these terms, as different from person to person, and from time to time.
Second, the formal definition of pain has finally introduced a conceptual wedge between ‘pain’ and ‘nociception’. The confusion, which is long-standing, and which has obfuscated scientific communication about how pain works, lies in the conceptual linkage of sensory perception with pain perception. Nociception, deriving from the Latin nocēre, suggests that the nerve endings in the body that detect external stimuli – the cutting, burning, or compression of the skin, for example – are pain detectors. Those nerves then send ‘pain signals’ to the brain, which responds. This is based on an understanding of nocēre as ‘to hurt’, when it might more usefully be translated as ‘to damage’. Those nerves detect damage, and they send damage signals, but damage does not imply pain. Only when damage signals reach the brain does the brain produce pain, if the circumstances are right for such a production. By no means do all damage signals result in the experience of pain. The formal separation of pain and nociception is useful because it puts an end to the notion that pain is formally correlated with injury. I will return to this at much greater length.
The third qualification here is also useful but requires further revision. It is important to acknowledge that people learn what pain is: that it is not a simple human universal to which everyone has the same access; it is a complex human variable that is accessed in all manner of ways, according to place, time, and other intersectional criteria. The further implication attached to this conceptual learning process is that there is not one thing called ‘pain’, but many different pains, each according to the way in which life experiences unfold. I seek to understand what is precisely meant by the phrase ‘life experiences’, how they are formed, and how they might change over time.
Fourth, regarding subjective reporting of pain, this is an important step forward in wresting formal control of the definition, diagnosis, and treatment of pain from the hands of doctors and placing it instead in the hands of patients. The modern history of an objective science or measurement of pain is the history of either ignoring or amplifying subjective reporting of people in pain, and is revealing of the unseemly history of racism, misogyny, classism, and ageism within the medical and allied professions. It should be enough for the medical establishment to endorse subjective reports of pain as truthful accounts of the experience of pain. As this book will illustrate, this has not typically been the case.
The word ‘usually’ in the fifth qualification could be struck because it is counterproductive. It is widely acknowledged that one of the biggest challenges facing medicine is the prevalence of chronic pain syndromes, which fall precisely into that category of bringing ‘adverse effects’ to the people who suffer from them. The need to cling to the idea of pain as adaptive is related to other medico-historical impetuses to try to know pain objectively and positively; to explain pain in ways that accord with the scientific need for natural laws. This is not to say that there is not an adaptive role for pain in evolutionary terms, but that the acknowledgement of the social and subjective construction of pain tends to make allusions to such rigid categories of analysis as ‘natural selection’ moot. In practice, both the experience of pain as suffering and the encounter of the medical community with people in pain fall into the category of dealing with ‘adverse effects’.
The sixth and final definitional caveat is a good one, disrupting the assumption that pain experience can only be gauged through pain utterances. Many scholars have pointed out that such utterances are, paradoxically, both extraordinarily rich and yet somehow inadequate in putting pain experience into the world. Several questions arise from this: if language is not the be all and end all of pain signs, what are the other signs and how does anyone know how to read them? If pain is social, personal, subjective, based on conceptual learning and life experience, how can the pains of others be accessed? It seems a difficult task when considering another human being, presenting in the clinic. What if the person is an historical figure, reachable only through the vagaries of a partial archive? What if the pained subject is not a person at all? How do we assess or come to know the pain of an animal, without resorting once again to the scientific temptation to objectify or to project?
Sense and Emotion
As a form of experience, pain is affectively produced.5 It has no direct or predictable relation to sensation, but where sensation is involved it is only through the construction of meaning that the sensations can be experienced as pain. This admixture of sensation and meaning-making involves an emotional repertoire: emotions, too, are meaningful ways of making sense of what is happening. Without meaning there is no pain. In effect, this means that without the meaningful interpretation of the senses and without emotion there is no pain. This observation is not new. It has been argued by physicians based on first-hand experience with patients;6 it has been argued by pain scientists researching the physiology and neurology of painful phenomena;7 it has been argued by neuroscientists looking for the similarities in the brain between pain associated with physical injury and suffering arising from social injury (hurt feelings, if you will) and by cultural psychologists trying to break out of the laboratory silo;8 it has been proven, by oblique means, by looking at the phenomenon of pain asymbolia or congenital analgesia, in which people experience injury consciously but attach no meaning to it and therefore do not experience it as pain.9 Psychologists, philosophers, anthropologists, and historians join the ranks of pain experts who acknowledge this fundamental affective dimension of pain. Not all of them follow its logical implications, but as a rule, the loose agglomeration of disciplines that makes up ‘pain studies’ agrees that pain is only pain if it is meaningfully and affectively produced. For all intents and purposes, the expression of a painful experience – whether the plaintive scream; the shedding of tears; the sharp intake of breath; stopping suddenly in your tracks; screwing up your face in a certain way; writhing (there is no limit or universality to such signs) – is an emotional experience, connected to the context in which it occurs, according to the expressive repertoire of the person in pain, according in turn to their own accretion of experience. It is bewildering to admit that despite a general multidisciplinary consensus, across vast schools of thought, about how to begin to think of pain, and how to come to know it, there remains an intractable urge among certain medical authorities to think of pain only in terms of a mechanical and automatic sensory function. There is also a huge communication gap about what pain is with the lay public at large. The equation of pain with the affective productions of the brain in relation to the world might be understood as tantamount to saying that the pain is ‘all in your head’. However much one might try to explain the profound complexity of the relationship between the brain, the nervous system, and the world from which meaning is derived, that it is not – or not necessarily – a dismissal but a means of unlocking the variety and mutability of pains, this is a difficult thing to sell. Most people, especially in moments of pain, or in their long-endured sufferings, want to hear about what can be done for their finger, or for their back, because, somehow in a common-sense way, it must be a structural or a functional problem; it must be an injury; it must have a place. It must be something’s fault. To say that pain is in the world, or between the world and you, seems like an intellectual abstraction. But pain does lie in between in this way.
If you cut your finger, you feel the pain there, and you staunch the bleeding there, and you cleanse and bandage there, and these acts, on the spot, help ease the pain. The bandage, just like the rubbing of a banged shin, or the kissing-better of tumbled toddler, is itself a salve. Its effect seems to take place at the point where it hurts. In the chapter on placebo, I’ll explain the complex relationship between belief and expectation and the internal pain-killing system that makes this magic work. But people do know, on an everyday practical level, that this kind of inter-relational social and material behaviour does in fact help, and from this can be gleaned the essence of the reality of pain. Mere damage is not pain. Damage is painful only when attached to meaning. Meaning, produced by the brain, is derived from the world. For the same reasons, feeling better is meaningfully derived from this dynamic relation of brain and world. It is about feeling beyond the narrow sensory definition, at the entanglement of sensory information with emotional experience, knowledge, and an appraisal of the contextual situation. These are integrated systems but they are unstable, largely unpredictable, and can be understood only by a multipronged approach that understands that the brain-body in pain is never isolated from the world in which pain has meaning.
This is still only a part of the pain-is-emotion story. I mentioned ‘hurt feelings’ already, and I want to underscore this point. While modern medicine, in its pain research, has overwhelmingly focused on the wound, on sensitivity, on damage in the body or dysfunction in the nervous system, much can be gained by an understanding of emotional pain – grief, exclusion, depression, despair, anxiety, Angst, sometimes fear and anger – as pain. The late-modern understanding of the affective quality of pain suggests that researchers look in this direction, but there remains a kind of divide between pain that is the purview of medicine and ‘pain’ that is social, the purview of culture, family, community, or self-reflection. The division is unhealthy and unhelpful, which is not to say that all these emotional conditions and an endless array of others in situated historical contexts should become the purview of medicine. Rather, the boundaries of the medical and the medical-scientific should be open, porous, alive not only to the physical body and the functions of the brain and the nervous system, but also to the possibilities of learning something from coming to know pain in its infinite cultural varieties. This knowledge, of pain as emotion, must disrupt pain knowledge per se.
My intention, as already stated, is to historicize pain. My approach to this topic has been formed by many years working in the field of the history of emotions. The premise of this field of study is that emotions have a history: they change over time; they have origin points and some disappear altogether; they are culturally and temporally specific; they are always present, even when – in the realm of political debate, law, science – it has been politically expedient to argue that they are not. Emotions are not merely the affective consequence of the unfolding of events, but causal, effectual parts of chronicity. I refer the reader to the relevant literature instead of expounding on this at length.10 Suffice to say that if emotions are historical and pain is an emotion, then pain is historical too. Its history can be accessed via the same methods as other works in the history of emotions: through an understanding of the plasticity of the brain and body and their dynamic relationship with the specific, situated world in which they are caught. This is a study of pain contexts, pain conceptual repertoires, situated pain experience – how it felt – and situated pain meanings. It is about language, material culture, belief systems, and knowledge just as much as it is about the brain and the body.
The book is written as a history, but pain studies is both intellectually and practically a multidisciplinary affair. What we know about pain is always situated, and I am constantly running contemporary epistemologies of pain against their forebears and asking questions of the ways in which knowledge is produced and changes over time. Critically, however, contemporary pain studies increasingly includes the testimony, experiences, expressions, and opinions of people in pain.11 It has enlivened a field of study by connecting formal frameworks of knowledge to often creative forms of putting pain into the world, which in turn has helped change and develop those formal frameworks of knowledge and suggested new forms of care and relief. In many ways, this openness, which starts with the opening of academic studies of pain to vastly different disciplinary approaches – biological, psychological, sociological, anthropological, historical – and flourishes with the inclusion of patient-led practices of management and protest, has been a perfect demonstration of the ways in which what is known about pain and how pain can be experienced can change in real time. It emphasizes the dynamic relation of knowledge and experience: what is known frames what is experienced, but access to experience can frame new knowledge. A new practice or expression might lead to a new feeling, which, if properly harnessed, might produce a new theory that can lead to the formalization of new therapies. It was, I will argue, ever thus, but that relationship is much easier to see now than it was in many historical contexts. All that is available to the historian, often, is the record of knowledge formalized in canonical works of medical authority. The experiential must be inferred. No one discipline can be master of this kind of holistic analysis. No one discipline can call the shots, whether it concerns what pain is, how it works, how to treat or prevent it, how to read or measure it, or how it feels.
I want to stress the necessary disruption of any implicit notion of a disciplinary hierarchy here. Pain studies is, or should be, a truly interdisciplinary affair. There are not pain sciences and then ‘softer’ pain humanities. There is no pain science without the crucial work of the humanities and social sciences that helps complete the picture of pain’s experiential contingency. I make no attempt to hide or otherwise obfuscate my own disciplinary background and training, but I make a concerted attempt to draw together diverse threads. In so doing, it sometimes becomes apparent where the interdisciplinary production of knowledge about pain is dysfunctional. Knowledge does get produced on parallel and even on divergent tracks, such that what we know about pain becomes paradoxical. As different disciplines claim incompatible truths, it is essential that probable errors all around are addressed. The primary error, in almost all cases, is the assumption, often unrealized, that a particular disciplinary approach is all that is required to unlock the secrets or solve the problems of pain.
Given the interdisciplinary scope, I have eschewed a typical historical narrative. I favour neither a chronological sequence nor a place-based focus, and the book is not limited to one period or to a regular notion of periodization. The coverage is global, from antiquity to the present, encompassing many different languages and cultures. Sometimes there is theoretical or thematic overlap; sometimes there are sharp distinctions and departures. The broad scope is reined in by thematic staging and by specific episodes of either source-based analysis, context-based analysis, or focused histories of sub-themes. Within each chapter, therefore, the reader can expect to find great leaps over time and across space. The point isn’t to be comparative or to show consistency across history. Rather, it is to exploit a certain historical method to show that it is possible, however partially, to uncover the relationship between pain knowledge and pain experience, and to exemplify elements of this method as the circumstances demand. My sources, therefore, are especially diverse: paintings, pottery, sculpture, photographs, diagrams, diaries and other ego narratives, letters, epic poetry, medical and scientific texts and treatises, a corporal-punishment device, novels, film, and a basilica. I have heard the charge that historians of emotions, senses, and experience are, despite their best intentions, essentially no different from cultural historians. To whatever extent they claim to be historicizing feelings and sensations, they are primarily researching in the realm of text, the word, what people said about what they felt. I hope to show by this approach that there is rather more to it than this. The word, the linguistic concept, is vital to the argument of this book – it deals in pain concepts in, I think, sixteen languages, to the meanings of which I have tried to be contextually faithful – but it is not the only important element. Through this wide array of sources, I aim to recover the body in pain, the lived experience of pain, and the richness of the history of communicating pain – putting it in the world – beyond the word.
Notes
1
Rob Boddice and Bettina Hitzer, ‘Emotion and experience in the history of medicine: elaborating a theory and seeking a method’, in
Feeling Dis-ease in Modern History: Experiencing Medicine and Illness
, eds Rob Boddice and Bettina Hitzer (London: Bloomsbury, 2022), 3–19.
2
Excellent recent examples of the history of pain include: Joanna Bourke,
The Story of Pain: From Prayer to Painkillers
(Oxford: Oxford University Press, 2014); Javier Moscoso,
Pain: A Cultural History
(Houndmills: Palgrave, 2012); and Rachel Ablow,
Victorian Pain
(Princeton: Princeton University Press, 2017).
3
John Bonica, ‘The need of a taxonomy’, and H. Merskey et al., ‘Pain terms: a list with definitions and notes on usage’,
Pain
, 6 (1979): 247–52, at 250.
4
Srinivasa N. Raja et al., ‘The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises’,
Pain
, 161 (2020): 1976–82, at 1977.
5
Rob Boddice, ‘Hurt feelings’, in
Pain and Emotion in Modern History
, ed. Rob Boddice (Houndmills: Palgrave, 2014), 1–15.
6
Ronald Melzack and Patrick Wall,
The Challenge of Pain
(London: Penguin, 1996), 15–18; Patrick Wall, ‘Introduction to the fourth edition of
Textbook of Pain
’,
Topical Issues in Pain
, 4 (2013): 7.
7
Serge Marchand, ‘The physiology of pain mechanisms: from the periphery to the brain’,
Rheumatic Disease Clinics of North America
, 34 (2008): 285–309.
8
N.I. Eisenberger, M.D. Lieberman, and K.D. Williams, ‘Does rejection hurt? An fMRI study of social exclusion’,
Science
, 302 (2003): 209–92; Lucas B. Mazur, ‘The importance of cultural psychological perspectives in pain research: towards the palliation of Cartesian anxiety’,
Theory & Psychology
, 32 (2022): 183–201.
9
Nikola Grahek,
Feeling Pain and Being in Pain
, 2nd edition (Cambridge, MA: MIT Press, 2007).
10
Jan Plamper,
The History of Emotions: An Introduction
(Oxford: Oxford University Press, 2015); Rob Boddice,
The History of Emotions
(Manchester: Manchester University Press, 2018).
11
Deborah Padfield and Joanna M. Zakrzewska, eds,
Encountering Pain: Hearing, Seeing, Speaking
(London: UCL Press, 2021).
ONEScriptingThe Politics of Knowledge
What is beyond and what is behind the process of defining pain? How has knowledge about pain been produced, developed, and disseminated? Knowledge is never produced neutrally. It always serves someone. Something is always at stake. There are always inclusions and exclusions, whether wilful or not. Knowledge is political and pain exemplifies this. This chapter examines the politics of knowledge from the point of view of medical authorities, probing at the formation of experiential frames of reference from antiquity to modernity. It is about the politicization of pain knowledge on several fronts. First, it documents the formation of one strand of historical pain scripts, which have roots in Greek antiquity and a distinctive historical development in early medieval Persia, and from there to medieval Spain and then throughout Europe. To complement the Greek and Arabic schools, I examine the canon of traditional Chinese medical knowledge on pain. In all cases, I am mindful of the ways that formative scripts – the most significant medical canons of pain knowledge – have later been erased by the cultural authority of modern medicine. The logics of ancient and medieval medicine have been overridden in the name of either connecting the knowledge claims of historical medical authorities with or disconnecting them from the knowledge claims of contemporary medicine. Throughout, I connect the formalization of pain knowledge to the way that the experience of pain was scripted. It does not matter so much who was right and who was wrong – this would even be a misdirection – for the experience of pain takes place within the epistemological framework that exists.
From Greek Pain to Arabic Pain
Bleeding as pain therapy was remarkably long-lived, stemming from time immemorial until the nineteenth century as a central pillar of medical practice, and lasting until today for specific cases. In its classical form, as iterated by Hippocrates and Galen, it was a central therapeutic strategy in alignment with humoral and meteorological understandings of human anatomy, function, and disease. The human temperament (the word literally refers to the specific mixture of the humours) was dependent on the balance of humoral substances: melancholy or black bile (cold and dry), yellow bile or choler (warm and dry), blood (warm and moist), and phlegm (cold and moist). The predominance of one humoral substance in the body over the others was indicated in the corresponding four types of temperament: melancholic, choleric, sanguine, phlegmatic. A pathological imbalance of the humours was caused by climatic conditions or food or activities that were out of accord with a person’s temperament. It is possible that the idea behind these four humours came from what happened to blood when it was separated out – something that can now be done by putting a vial of blood in a centrifuge. Melancholy, for example, would appear as a darker substance at the bottom of the tube – in fact, clotted blood. When the four humours were in balance in the body, which is to say, in proportions correct to each other, then the person was healthy and well disposed. If the humours were out of balance, this was the cause of disease. In the case of general excess of all the humours (plethora), balance could be restored by bleeding. One sign of excess was pain. If the humour-containing vessels were distended by a plethora of substance, leading ‘to a feeling of tension, soreness or pain’, then relief was to be achieved by bleeding, among other therapies according to the patient’s age, strength, and even the time of year.1
Galen was born in Pergamon, situated in what is now the west of Turkey, near the Aegean Sea, in 129 ce, and died in about 216. The shadow of his medical influence falls across a millennium and a half and cannot be overstated. Galen’s innovation concerning pain was to connect sensory perception to the brain, that is, to the cognitive processing of sensory information, such that the subject becomes aware of it. Under that generality, there were numerous causes of pain, all of them related to the specific balance or imbalance of the humours and their specific qualities. To this extent, Galenic pain is sensory, physical, nervous, cognitive, and affective, but all of these terms risk anachronism, for pain according to Galen pertains to the qualities of humours and to the location of the soul in the brain, and to the physical relation of the former and the latter. Inflammation was one cause of pain; physical injury (discontinuity) was another; and there was room for something like psychosomatic pain, where pain in a certain part of the body is unrelated to imbalance, inflammation, or injury of that part. There is, in Galen’s apprehension of the process of pain, a notion of a kind of nervous pathway, between an affected part and the brain, but it is only in the brain’s reception of sensory information that pain is perceived.2 In any case, ancient Greek concepts of pain, suffering, and toil – ἄλγος (álgos), λῡ́πη (lū́pē), ὀδύνη (odúnē), πᾰ́θος (páthos), and πόνος (pónos) – could all indicate both the physical and mental aspects of pain, situated in a general understanding of the passions that did not (could not) attempt to disentangle affective phenomena from bodily phenomena. While Greek culture had complex notions of the division of the soul and the body’s relation to it, the mind–body dualism that has been the hallmark of modernity would have been alien to Galen and to the hundreds of years of Greek civilization that preceded him.3
How could a medical man access the experience of someone in pain, whether for diagnostic or therapeutic purposes? How could pain be known and shared? To some extent, Galen understood that people experienced pain in common with other people. Courtney Roby calls it an ‘experiential consensus’.4 Yet at the same time, he mistrusted a patient’s capacity to make sense in verbal terms of a pain sensation, or to correctly describe what was happening in their own body. Galen set about delimiting the descriptive categories of pain to avoid slippages that obfuscated the experience, its bodily location, and its medical implications. While Roselyne Rey highlighted four broad categories of pain that were operative for Galen – throbbing (or pulsating), weighty or heavy, stretching and lancinating – there were many other types of pain that he abided by on the basis that they were ‘so widely known’ they required no ‘special explanation’: pricking pain (νυγματώδη), tearing (stretching) pain (διατείνοντα), violent or vehement pain (σφοδρòν), severe or powerful pain (ἰσχυρòν), violent or forcible pain (βίαιον), constant or continuous pain (συνεχῇ), and intermittent pain (διαλειποντα). That this list contains numerous ‘or’ words is testimony to the vagaries of translation, but in terms of physical description, Galen’s typology of experienced pains sound familiar enough.5 Yet all these types of experience must be situated within both the patient’s and the medical authority’s understanding of cause (humours) and therapy (bleeding, often), such that the experience is likely some distance from the closeness that translation tends to imply. Besides this, there is a whole culture of painful experience outside of the medical purview that nonetheless inflects the medicalized ‘experiential consensus’. I refer back to this culture at various points throughout the book.
The Galenic tradition was preserved, yet altered, in the medieval Persian world of Ibn Sina (Avicenna to the Europeans), whose medical Canon juggled Galen and a host of other medical expertise, from India and China, and from his own immediate culture. Hellenistic influence in Persia is well documented, and all the available Greek works of medicine were in Arabic translation by the early eleventh century ce.6 While this involved the creation of formal Arabic terminology, by the time of Ibn Sina this was well established. The Canon was written over at least a decade, in the cities of Ray (now a part of Greater Tehran) and Hamadan (mid-western Iran), and published in 1025. Until the Greek revival of the sixteenth century in Europe and, for many, long afterwards, Ibn Sina remained the principal medical authority, with the Canon the main medical text. While agreeing in broad principles with Galen about the ways in which pain was carried to the brain (not the heart), Ibn Sina nonetheless has been understood in recent scholarship to have expanded the causes of pain from injury to temperamental changes (any sudden change, for example in temperature, could cause pain, as could sudden change in the mixture of the humours in a particular organ) and to have expanded the number of types of pain from Galen’s four to fifteen. It should be noted that Galen himself drastically reduced the number of medically viable pain descriptors that he had found in Archigenes, on the basis that they were unintelligible and confusing, but, as already noted, it is incorrect that Galen reduced the typology of pain to four types.7 In some instances (numbness, for example), Ibn Sina restored a category of ‘pain’ that Galen had explicitly rejected. Scholars have gone to great lengths to try to map Ibn Sina’s pain categories onto contemporary descriptions of pain (others have done the same for Galen), such that they might even foreshadow the classificatory system of the McGill Pain Questionnaire (explored at length in chapter 4 on chronic pain).8 This is to be indulgent in translation, perhaps, and to play fast and loose with situated meanings, for all of the types of Ibn Sina’s ‘pain’, and Galen’s too, were based upon a humoral understanding of human physiology. The implication, according to the antihistorical tradition of joining straight lines between Ibn Sina’s knowledge and contemporary medical knowledge, is that a pain description served a particular experience of pain that, the underlying context of the description notwithstanding, does not change. The analysis cannot work. The category of ‘pain’ that appears in both Galen and Ibn Sina is a broad category that includes feelings and symptoms that most contemporary medical authorities would not class as pain at all.
I have tried – through a reading of Ibn Sina’s ‘pain’ categories in Arabic that has no a priori agenda to connect them to anything like present-day pain categories – to arrive at the situated meanings of these terms, resisting the temptation to label each one as ‘pain’.9 In the list and description of these categories in Ibn Sina, each one is marked as a type of Wajaʿ, which could be translated as ‘pain’, hurt, ache, or disease, or, per Ibn Sina’s own definition, ‘a feeling of incongruity’.10 Most scholars acknowledge this breadth of meaning, yet obscure it by insisting on listing types of ‘pain’. Instead, I list a range of them here as categories of dis-ease – a term that perhaps more neatly captures this notion of a feeling of incongruity, and which preserves the latitude of medieval ‘pain’ as encompassing troublesome and discomforting experiences that go beyond physical hurt. In each case, I give the Arabic transliteration with original script in parentheses, followed by the Farsi transliteration and original script, followed by its meaning in English.
The first named dis-ease, telling enough for the point I wish to make, is Wajʿ-i-hakkāk (الوجع الحکّاک), Dard-e Khāreshī (درد خارشی), meaning ‘itchy’. The Arabic might indicate something like scraping or chafing sense of harm, a sensation of friction, but it makes sense simply to settle on the feeling of itchiness. Most scholars prefer ‘itching pain’, but I do not think this should apply. It is caused here by acrid or sharp humours and treated accordingly. Once we remove the need to translate Wajʿ into a narrow definition of ‘pain’, the meaning of an itchy discomfort emerges. It appears in a general list that includes things recognizable as physical pain because it shares in an aetiological explanation: the humours.11
The second dis-ease is Wajʿ-i-khashin (الوجع الخشن), Dard-e Zebrī (درد زبری), which is often translated as ‘irritating pain’. The circularity of the textual description does not help much, since it advises that this kind of pain is caused by this kind of humour, so it is important to know what khashin means: rough or raw or rude. Something unrefined in the humoral condition equates to something similar in the character of the experience. Is it ‘irritating’? Maybe. But that doesn’t seem to get to the heart of the intended meaning. The Farsi indicates something rough or spikey. So, this is a feeling of roughness or rawness.
Wajʿ-i-nākhis (الوجع الناخس), Dard-e Khalande-h (درد خلنده), is often translated as ‘stretching pain’ or sometimes ‘tension pain’ (I suspect to fit with later Latin translations, and to fit with Galen, but see more on this below), but it seems to refer to a sting or prick. Again, there is circularity in the description of the cause, since this dis-ease refers to the action of a humour that has this quality of effecting the muscles and nerves. Wajʿ-i-momaddid (الوجع الممدَد), Dard-e Feshārī (درد فشاری), is pressure or compression, and could be a physical pain, but it could also be the experience of feeling compressed: of a weight bearing on a part.
One begins to see the point that these descriptions are both diminished and rendered confusing if it is insisted that they be made narrowly to conform to a modern western notion of pain. Rather, to understand them, it is necessary to relinquish this narrow understanding and to embrace a category of pain that is far broader, nearer to a sense of dis-ease. Two final examples clinch the argument. Ibn Sina’s Wajʿ-i-rikhw (الوجع الرخو), Dard-i Sost (درد سست), has been translated as ‘relaxing pain’ – most confusing – and could be something like a ‘soft’ or ‘loose’ ache, but it is the feeling of flaccidity that makes most sense. The Farsi is suggestive of looseness, but also numbness: a category that Galen had explicitly rejected as a type of pain, for reasons that are rather obvious. Something that is loose, relaxed, flaccid, or numb does not make sense as a pain, but it does make sense as a dis-ease. Ibn Sina’s text gives a precise circumstance for this loose feeling, in which a muscle is stretched but not the ligaments and tendons. One might be troubled by such a condition without experiencing pain. In a final example, Wajʿ-i-Iʿiyāiī (الوجع الإعیائی), Dard-i Khastigī (درد خستگی), often translated as ‘tired pain’ or ‘fatigue pain’, is simply a feeling of fatigue. While there is a temptation to connect this to the pains experienced in chronic fatigue syndrome, again this does not seem to be implied here. The cause is given as overwork, so why not simply understand this as it was intended: an uncomfortable feeling of tiredness?
How could it be that such a well-studied text has become so mangled in modern translation? There is, without question, a desire to connect Ibn Sina to modernity, to emphasize the profundity of his medical vision, but this is rather undermined (a) by the argument that his ‘pain’ categories map comfortably onto something like the McGill Pain Questionnaire and (b) by the fact that they contain such confusing examples as ‘relaxing pain’, ‘itching pain’, and ‘tired pain’. I suspect that the intention is compounded by a reading of Ibn Sina through its Latin translation.









