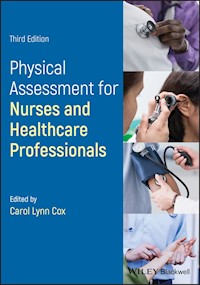
Physical Assessment for Nurses and Healthcare Professionals E-Book
44,99 €
Mehr erfahren.
- Herausgeber: John Wiley & Sons
- Kategorie: Fachliteratur
- Sprache: Englisch
Physical Assessment for Nurses and Healthcare Professionals offers a practical and comprehensive guide to best clinical practice when taking patient history and physical examination. This accessible text is structured in accordance with the competencies for advanced practice in assessment, diagnosis and treatment as published by the RCN. Following a systematic, systems-based approach to patient assessment, it includes a summary of the key clinical skills needed to develop and improve clinical examination in order to confidently assess, diagnose, plan and provide outstanding care.
In this revised edition, colour photographs and case studies have been included to assist health care practitioners in their assessment of the patient. This important guide:
- Includes a highly visual colour presentation with photographs and illustrations
- Features a wide range of key learning points to help guide practice
- Offers illustrative examples, applications to practice and case studies
Written for health care students, newly qualified and advanced nurse practitioners, and those in the allied health professions, Physical Assessment for Nurses and Healthcare Professionals is the essential guide for developing the skills needed to accurately access patient history and physical examination.
Sie lesen das E-Book in den Legimi-Apps auf:
Seitenzahl: 694
Veröffentlichungsjahr: 2019
Ähnliche




Table of Contents
Cover
List of Contributors
Foreword
Preface
Acknowledgements
Introduction: The First Approach
General Principles
Your Role as an Advanced Healthcare Practitioner
References
Chapter 1: Interviewing and History Taking
General Procedures
Functional Enquiry
Past History
Family History
Personal and Social History
References
Chapter 2: General Health Assessment
Introduction
General Inspection
Hands
Skin
Mouth
Eyes
Examine the Fundi
Examine for Palpable Lymph Nodes
Lumps
Heart
Breasts
Respiratory
Thyroid
Other Endocrine Diseases
Abdominal
Musculoskeletal
References
Chapter 3: Examination of the Skin, Hair, and Nails
Introduction
Anatomy and Physiology
Conclusion
References
Chapter 4: Examination of the Cardiovascular System
Introduction
General Examination
Palpate the Radial Pulse
Take the BP
Jugular Venous Pulse (Frequently Called Pressure)
Musset's Sign
The Precordium
Auscultation
Signs of Left and Right Ventricular Failure
Functional Result
Summary of Common Illnesses
Peripheral Arteries
Varicose Veins
System‐Oriented Examination
Reference Guide: Intracardiac Values and Pressures
References
Chapter 5: Examination of the Respiratory System
Introduction
Anatomy and Physiology
General Examination
Physical Assessment of the Chest
Inspection of the Chest
Palpation
Percussion
Auscultation
Vocal Fremitus/Resonance
Sputum
Functional Result
Summary of Common Illnesses
System‐Oriented Examination
References
Chapter 6: Examination of the Abdominal System
Introduction
Anatomy and Physiology
The Pancreas
The Liver
The Large Intestine (Colon)
Ascending Colon
Transverse Colon
Descending Colon
Sigmoid Colon
Rectum
Anal Canal
General Examination
Abdominal Pain
Inspection
Arterial Bruits
Liver and Gall Bladder
Spleen
Groin
Hernia
Kidneys and Bladder
Aorta
Examination of Genitals
Digital Rectum Examination
Per Vaginam Examination
Summary of Common Illnesses
References
Chapter 7: Examination of the Male Genitalia
Introduction
General Examination
Inspection
Palpation
References
Chapter 8: Examination of the Female Breast
General Examination
Introduction
Review of Anatomy
Inspection
Palpation
Referral Guidelines for Breast Cancer
The Male Breast
References
Chapter 9: Examination of the Female Reproductive System
General Examination
Review of Anatomy
Preparation
Inspection of the External Genitalia
Speculum Examination (Figure 9.4)
Bimanual Examination
Female Genital Mutilation (FGM)
Overview of Common Presentations
References
Chapter 10: Examination of the Nervous System
General Examination
General Examination
Motor and Sensory Function
Mental Function
Skull and Spine
Cranial Nerves (I – XII)
Limbs and Trunk
Lower Limbs
Summary of Common Illnesses
References
Chapter 11: Examination of the Eye
General Examination
Examination
Recording Visual Fields
References
Chapter 12: Mental Health Assessment
Introduction
Motivational Interviewing (MI)
General History and Examination
Challenging Behaviour
Summary of Common Mental Disorders
Conclusions
Acknowledgements
References
Chapter 13: Examination of the Musculoskeletal System
General Examination
Frequent Musculoskeletal Complaints
Terms of Location
Terms Used to Describe ROM
References
Chapter 14: Assessment of the Child
General Examination
References
Chapter 15: Assessment of Disability Including Care ofthe Older Adult
General Examination
Assessment of Impairment
Assessment of Hearing
Assessment of Disability
Analysing Disabilities and Handicaps and Setting Objectives
Identifying Causes for Disabilities
References
Chapter 16: Imaging Techniques, Clinical Investigations, and Interpretation
General Procedures
Diagnostic Imaging
Endoscopy
Needle Biopsy
Cardiac Investigations
Respiratory Investigations
Gastrointestinal Investigations
Renal Investigations
Neurological Investigations
Further Reading
Chapter 17: Basic Examination, Notes, and Diagnostic Principles
Basic Examination
Example of Notes
Problem List and Diagnoses
References
Chapter 18: Presenting Cases and Communication
Presentations to Healthcare Professionals and Patients
People – Including Patients
Diabetes Case
References
Appendices
Appendix A: Jaeger Reading Chart
Reference
Appendix B: Visual Acuity 3 Meter/21 Foot Chart
Reference
Appendix C: Hodkinson Ten‐Point Mental Test Score
Reference
Appendix D: Barthel Index of Activities of Daily Living
Guidelines for the Barthel Index of Activities of Daily Living (ADL)
Reference
Appendix E: Mini‐Mental State Examination (MMSE)
References
Appendix F: Glasgow Coma Scale
Reference
Appendix G: Warning Signs of Alzheimer’s Disease
Reference
Appendix H: Trigger Symptoms Indicative of Dementia
References
Index
End User License Agreement
List of Tables
Chapter 2
Table 2.1 Distribution of components in the four imaginary quadrants of the a...
Chapter 3
Table 3.1 Skin types.
Table 3.2 Systemic disease.
Table 3.3 Distribution of lesions.
Table 3.4 Primary lesions.
Table 3.5 The shape and border of lesions.
Table 3.6 Secondary lesions.
Table 3.7 Contact and allergic dermatitis.
Table 3.8 Tinea infections.
Chapter 4
Table 4.1 Intracardiac values and pressures.
Chapter 5
Table 5.1 Discrimination of sounds.
Table 5.2 Characteristics of sounds.
Chapter 9
Table 9.1 Materials needed for a pelvic examination.
Table 9.2 Differential diagnosis of acute pelvic pain.
Chapter 10
Table 10.1 The brain.
Table 10.2 Spinal nerves.
Table 10.3 SOCRATES.
Table 10.4 Glasgow Coma Scale.
Table 10.5 ‘Examine the cranial nerves’.
Chapter 12
Table 12.1 Common actuarial measures and their predictive efficacy (Abderhald...
Table 12.2 Common actuarial risk measures and their effect sizes.
Chapter 14
Table 14.1 Approach to history taking – age‐related history.
Table 14.2 Differences in anatomy and physiology.
Table 14.3 Developmental considerations affecting the physical assessment.
Table 14.4 Developmental approach to the physical assessment.
List of Illustrations
Chapter 1
Figure 1.1 Usual sequence of events.
Chapter 3
Figure 3.1 The skin.
Figure 3.2 Diascopy.
Figure 3.3 Nodular basal cell carcinoma.
Figure 3.4 Squamous cell carcinoma.
Figure 3.5 Malignant melanoma.
Figure 3.6 Toxic erythema.
Figure 3.7 Erythema multiforme.
Figure 3.8 Erythema nodosum.
Figure 3.9 Erythroderma.
Figure 3.10 Atopic eczema.
Figure 3.11 Contact dermatitis.
Figure 3.12 Impetigo.
Figure 3.13 Eczema herpeticum.
Figure 3.14 Hand, foot, and mouth disease.
Figure 3.15 Pityriasis rosea.
Figure 3.16 Plaque psoriasis.
Figure 3.17 Pustular psoriasis.
Chapter 4
Figure 4.1 Xanthelasma.
Figure 4.2 Xanthoma.
Figure 4.3 Taking a radial pulse.
Figure 4.4 Waveform of the pulse.
Figure 4.5 Taking the blood pressure and types of equipment that can be used....
Figure 4.6 Assessing height of JVP.
Figure 4.7 The veins of the neck.
Figure 4.8 Assessing the JVP waveform.
Figure 4.9 Location of PMI at the apex.
Figure 4.10 (a) Midsternal. (b) Midclavicular. (c) Anterior axillary.
Figure 4.11 Palpation position for right ventricular heave.
Figure 4.12 Ausculation site landmarks.
Figure 4.13 Relationship of heart sounds to the electrocardiogram.
Figure 4.14 Relation of murmurs to pressure changes and valve movements.
Figure 4.15 (a) Normal and (b) paradoxical splitting.
Figure 4.16 Radiation of sound from turbulent blood flow.
Figure 4.17 Diastolic murmurs in mitral stenosis.
Figure 4.18 Stages of mitral valve prolapse.
Figure 4.19 Sites of peripheral pulses.
Figure 4.20 Healing varicose ulcer – classic site in lower leg medially with ...
Figure 4.21 Site of systolic bruit in aortic aneurysm.
Chapter 5
Figure 5.1 Anterior and posterior landmarks to locate the lungs.
Figure 5.3 Anterior and posterior landmarks to locate the lungs.
Figure 5.4 Demarcation lines of the thorax. (a) Midsternal line; (b) Midclavi...
Figure 5.6 Demarcation lines of the thorax. Reproduced with permission.
Figure 5.7 Percussion sequence of the chest.
Figure 5.8 Percuss the diaphragm from above downwards. These markings are at ...
Figure 5.9 Determination of diaphragmatic excursion.
Figure 5.10 Sequence for auscultation.
Figure 5.11 Auscultation of adventitious sounds.
Chapter 6
Figure 6.1 Spider naevi in cirrhosis – telangiectasia radiating from central ...
Figure 6.2 Virchow's node.
Figure 6.3 Spider naevus: a small collection of capillaries fed by a central ...
Figure 6.4 William Harvey's method of checking vein filling.
Figure 6.5 Nine abdominal quadrants and location of organs in epigastric, hyp...
Figure 6.6 Auscultation sites for arterial bruits.
Figure 6.7 Examination of the liver.
Figure 6.8 Splenic enlargement.
Figure 6.9 Shifting dullness.
Chapter 7
Figure 7.1 The male reproductive system.
Figure 7.2 Longitudinal section of the penis and its relationship to the blad...
Figure 7.3 Checking for hernia.
Figure 7.4 The prostate.
Chapter 8
Figure 8.1 Anatomy of the female breast.
Chapter 9
Figure 9.1 Female reproductive system.
Figure 9.2 The internal female reproductive organs.
Figure 9.3 External female genitalia.
Figure 9.4 Speculum examination.
Figure 9.5 Bimanual examination.
Chapter 10
Figure 10.1 The brain.
Figure 10.2 Cerebral blood supply.
Figure 10.3 Nerve and action potential.
Figure 10.4 Action potential.
Figure 10.5 Node of Ranvier.
Figure 10.6 Testing temporal peripheral patient fields of vision.
Figure 10.7 Visual field assessment.
Figure 10.8 Visual field defects.
Figure 10.9 Accommodation reflex.
Figure 10.10 Muscles of the eye and relevant cranial nerves.
Figure 10.11 Testing external ocular movements (EOM)
Figure 10.12 Left 6th nerve lesion.
Figure 10.13 Concomitant nonparalytic strabismus.
Figure 10.14 Supranuclear palsies.
Figure 10.15 Cerebellar nystagmus.
Figure 10.16 Assessment areas for trigeminal nerve sensation.
Figure 10.17 The corneal reflex.
Figure 10.18 Fifth nerve palsy.
Figure 10.19 Jaw jerk test.
Figure 10.20 Upper and lower motor neuron lesions.
Figure 10.21 Rinne's and Weber's tests.
Figure 10.22 Stimulating the gag reflex.
Figure 10.23 Flexing the neck and raising both shoulders.
Figure 10.24 Left hypoglossal lesion.
Figure 10.25 Tapping both arms downwards.
Figure 10.26 Testing coordination – index finger to nose.
Figure 10.27 Cerebellar function – index finger to nose to examiner's moving ...
Figure 10.28 Testing muscle power.
Figure 10.29 Testing power: shoulder abduction and elbow flexion.
Figure 10.30 Tendon reflexes.
Figure 10.31 Trunk reflexes.
Figure 10.32 Lower limb coordination.
Figure 10.33 Muscle power in the legs. Hip flexion.
Figure 10.34 Knee flexion.
Figure 10.35 Testing knee reflexes.
Figure 10.36 Testing ankle jerk.
Figure 10.37 Plantar response stimulus.
Figure 10.38 Testing position sense.
Figure 10.39 Dermatomes.
Figure 10.40 Parkinson's disease gait.
Figure 10.41 Spastic gait.
Figure 10.42 Sensory ataxia gait.
Figure 10.43 Cerebellar gait.
Figure 10.44 Romberg's test.
Figure 10.45 Anatomy and vascular supply of the spinal cord. Note: Anterior s...
Figure 10.46 Signs of meningeal irritation.
Figure 10.47 Straight‐leg raising for sciatica.
Figure 10.48 Wasted interossei and hypothenar eminence from an ulnar nerve or...
Figure 10.49 Radial, median, and ulnar nerve palsies.
Chapter 11
Figure 11.1 The Eye.
Figure 11.2 Kay Picture Charts.
Figure 11.3 Slit lamp.
Figure 11.4 Examination of the retina with the slit lamp.
Figure 11.5 Alternative method for examination of the fundus.
Figure 11.6 Tonometer with diagram to illustrate correct alignment of the sem...
Figure 11.7 Retinoscopy
Figure 11.8 Corneal topography.
Figure 11.9 Phoropter.
Chapter 12
Figure 12.1 Healthy people 2020 – health determinants.
Chapter 13
Figure 13.1 The neutral position.
Figure 13.2 Movements of the neck.
Figure 13.3 (a) Thoracolumbar spine and sacroiliac joint. (b) Changes in the ...
Figure 13.4 Flexion and extension of the spine.
Figure 13.5 Straight leg raise with pain increased on dorsiflexion of the foo...
Figure 13.6 Further extension of the nerve root increases pain when the knee ...
Figure 13.7 Movements of the shoulder.
Figure 13.8 Shoulder abduction..
Figure 13.9 Movements of the elbows and shoulders.
Figure 13.10 Flexion and testing power of the elbow.
Figure 13.11 Movements of the wrist.
Figure 13.12 Flexion of the fingers.
Figure 13.13 Abduction of the fingers.
Figure 13.14 Movements of the hip, flexion and extension.
Figure 13.15 Movements of the hip, abduction and rotation.
Figure 13.16 Movements of the knee.
Figure 13.17 Testing power in the hand.
Chapter 16
Figure 16.1 Ultrasound scan showing a stone within gall bladder, casting an a...
Figure 16.2 (a) A normal
posteroanterior
(
PA
) chest radiograph; (b) An antero...
Figure 16.3 Outline of cardiothoracic structures that may be visualised on a ...
Figure 16.4 Outline of visceral organs that may be visualised on an abdominal...
Figure 16.5 Left coronary artery angiogram viewed from right.
Figure 16.6 Axial CT scan across cerebral hemispheres.
Figure 16.7 Magnetic resonance imaging.
Figure 16.8 (a) MRI (axial section) of the brain. The central white areas are...
Figure 16.9 Thallium 201 study of the heart.
Figure 16.10 The positioning of the limb electrodes and the six standard lead...
Figure 16.11 Example of a strongly positive exercise test – signal averaged r...
Figure 16.12 Outline of two‐dimensional echocardiograph (ultrasound scan). Ao...
Figure 16.13 Outline of M‐mode echocardiographs, with two examples showing mi...
Figure 16.14 Cardiac catheterisation.
Figure 16.15 Aortic stenosis. The systolic pressure falls as the catheter tip...
Figure 16.16 Mitral stenosis. Left ventricular (LV) pressure trace expanded t...
Figure 16.17 The arrangement for the 24‐hour ECG tape recorder.
Figure 16.18 Descriptive clinical terms. Shaded area is normal range.
Figure 16.19 Peak flow machine.
Figure 16.20 A vitalograph.
Figure 16.21
V/Q
scan of pulmonary embolism: (a) ventilation scan – normal; ...
Figure 16.22 Endoscopic retrograde cholangiopancreatography.
Figure 16.23 The lumbar puncture needle is positioned between L3 and L4 to on...
Guide
Cover
Table of Contents
Begin Reading
Pages
iii
iv
xvii
xviii
xix
xxi
xxiii
xxv
xxvi
xxvii
xxviii
xxix
xxx
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
149
150
151
152
153
154
155
156
157
159
160
161
162
163
164
165
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
415
416
417
418
419
420
421
422
423
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
Physical Assessment for Nurses and Healthcare Professionals
Third Edition
EDITED BY
CAROL LYNN COX PhD, MSc, MA (Theology) MA (Education), PG Dip Education, BSc (Hons), RN, ENB 254, FHEA
Professor Emeritus, School of Health Sciences, City, University of London, London, UKClinic Manager and Director of Nursing, Health and Hope Clinics, Pensacola, FL, USA
Adapted from Lecture Notes on Clinical Skills (third edition) by:
THE LATE ROBERT TURNER MD, FRCP
Professor of Medicine and Honorary Consultant PhysicianNuffield Department of Clinical MedicineRadcliffe Infirmary, Oxford, UK
ROGER BLACKWOOD MA, FRCP
Consultant Physician, Wexham Park Hospital, Slough, and Honorary Consultant Physician at Hammersmith Hospital, London, UK
This edition first published 2019 © 2019 by John Wiley & Sons LtdEdition History [2e, 2009]
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by law. Advice on how to obtain permission to reuse material from this title is available at http://www.wiley.com/go/permissions.
The right of Carol Lynn Cox to be identified as the author of editorial in this work has been asserted in accordance with law.
Registered Office(s)John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030, USAJohn Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial Office9600 Garsington Road, Oxford, OX4 2DQ, UK
For details of our global editorial offices, customer services, and more information about Wiley products visit us at www.wiley.com.
Wiley also publishes its books in a variety of electronic formats and by print‐on‐demand. Some content that appears in standard print versions of this book may not be available in other formats.
Limit of Liability/Disclaimer of WarrantyThe contents of this work are intended to further general scientific research, understanding, and discussion only and are not intended and should not be relied upon as recommending or promoting scientific method, diagnosis, or treatment by physicians for any particular patient. In view of ongoing research, equipment modifications, changes in governmental regulations, and the constant flow of information relating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate the information provided in the package insert or instructions for each medicine, equipment, or device for, among other things, any changes in the instructions or indication of usage and for added warnings and precautions. While the publisher and authors have used their best efforts in preparing this work, they make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation any implied warranties of merchantability or fitness for a particular purpose. No warranty may be created or extended by sales representatives, written sales materials or promotional statements for this work. The fact that an organization, website, or product is referred to in this work as a citation and/or potential source of further information does not mean that the publisher and authors endorse the information or services the organization, website, or product may provide or recommendations it may make. This work is sold with the understanding that the publisher is not engaged in rendering professional services. The advice and strategies contained herein may not be suitable for your situation. You should consult with a specialist where appropriate. Further, readers should be aware that websites listed in this work may have changed or disappeared between when this work was written and when it is read. Neither the publisher nor authors shall be liable for any loss of profit or any other commercial damages, including but not limited to special, incidental, consequential, or other damages.
Library of Congress Cataloging‐in‐Publication Data
Names: Cox, Carol Lynn, editor. | Based on (work): Blackwood, Roger. Lecture notes on clinical skills. 2003.Title: Physical assessment for nurses and healthcare professionals / edited by Carol Lynn Cox.Other titles: Physical assessment for nurses.Description: Third edition. | Hoboken, NJ : Wiley‐Blackwell, 2019. | Preceded by Physical assessment for nurses / edited by Carol Lynn Cox. 2nd ed. 2010. | Based on Lecture notes on clinical skills / Roger Blackwood, Chris Hatton. 4th ed. 2003. | Includes bibliographical references and index. |Identifiers: LCCN 2018044840 (print) | LCCN 2018045696 (ebook) | ISBN 9781119108986 (Adobe PDF) | ISBN 9781119108993 (ePub) | ISBN 9781119108979 (pbk.)Subjects: | MESH: Nursing AssessmentClassification: LCC RT48 (ebook) | LCC RT48 (print) | NLM WY 100.4 | DDC 616.07/5–dc23LC record available at https://lccn.loc.gov/2018044840
Cover Design: WileyCover Images: © Martin Barraud/Getty Images, © Hero Images/Getty Images, © XiXinXing/Getty Images, © Blend Images ‐ Jose Luis Pelaez Inc/Getty Images
List of Contributors
Daniel Apau, MSc (Advanced Practice), PG Dip, BSc (Hons), RN, FHEARegistered Nurse, Medical Intensive Care, Houston Northwest Medical Center, Houston, TX, USA
Michael Babcock, MDCollege of Medicine, Florida State University, Pensacola, FL, USA
Graham M. Boswell, D Ed, MA Ed, BA (Hons), BSc (Hons) RGN, FHEASenior Lecturer, Department of Adult Nursing and Paramedic Science, Faculty of Education and Health, University of Greenwich, London, UK
Carrie E. Boyd, MSN, BSN, RNStaff Nurse, Health and Hope Clinics, Pensacola, FL, USA
Patrick Callaghan, PhD, MSc, BSc (Hons), RN, FHEAProfessor of Mental Health Nursing and Chartered Health Psychologist
University of Nottingham and Nottinghamshire Health Care NHS Trust, Nottingham, UK
Carol Lynn Cox, PhD, MSc (Nursing), MA (Theology) MA Ed, PG Dip Ed, BSc (Hons), FD, RN, FHEAProfessor Emeritus, School of Health Sciences, City, University of London, London, UK
Clinic Manager, Health and Hope Clinics, Pensacola, FL, USA
Jennifer Edie, M Ed, MBA, TDCR, DMUSenior Lecturer, Department of Allied Health Professions and Midwifery, School of Health and Social Work, University of Hertfordshire, Hatfield, Hertfordshire, UK
Helen Gibbons, MSc, PG Cert (Medical Education), ENB (Ophthalmic Practice), BA (Hons), RNClinical Nursing Lead (Education and Research), Moorfields Eye Hospital NHS Foundation Trust, London, UK
Course Director, PG Cert Ophthalmic Practice, University College London, London, UK
Jessica Ham, MSN, BSN, ASN, FNP, RNClinical Preceptor, College of Medicine, Faculty of Florida State University, Tallahassee, FL, USA
Clinical Director, Elevate Personalized Medicine, Pensacola, FL, USA
Siobhan Hicks, MSc (Advanced Practice), PG Cert (Academic Practice), PG Cert (Leadership), BSc (Hons), RNAdvanced Nurse Practitioner, Andrews Health Centre, London, UK
Lecturer in Advanced Practice, School of Health Sciences, City, University of London, London, UK
Victoria Lack, MSN, PG Dip (Academic Practice), BN (Hons), FNP, Non‐Medical Prescriber, DN(Cert), RNLecturer in Primary Care, Department of Health Sciences, University of York, York, UK
Advanced Nurse Practitioner, Beech House Surgery, Knaresborough, North Yorkshire, UK
Brandy Lunsford, MSN, BSN, APRNClinical Director, Health and Hope Clinics, Pensacola, FL, USA
Anthony McGrath, MSc, PGCE, BA (Hons) RMN, RGN, FHEAPrincipal Lecturer, Head of Adult Nursing and Midwifery
London South Bank University, London, UK
Nicola L. Whiteing, MSc, PG Dip HE, BSc (Hons), RN, RNT, ANPLecturer in Nursing, Southern Cross University, Lismore, New South Wales, Australia
Foreword
Underpinning the appropriate delivery of healthcare is the Physical Assessment. This structured physical examination allows the healthcare professional to obtain a comprehensive assessment of the patient and is critically important in that it leads to clinical decisions which are crucial for the patients' care.
This volume, Physical Assessment for Nurses and Healthcare Professionals, provides a clear and easy‐to‐use guide to achieving an excellent physical assessment. It is specifically intended for those embarking on a career in healthcare and contains the techniques used by specialist/advanced practitioners.
In this book the need for a comprehensive and holistic approach to the Physical Assessment is excellently presented by Professor Cox. Professor Cox shows how important it is to develop a rapport with the patient in order to carefully assess their perceptions and how this relationship must be established from the very first meeting when information is exchanged between the healthcare professional and the patient. Fundamental to gaining this perspective is to listen. The importance of guiding the healthcare practitioner to engage in active listening cannot be underestimated and this is reflected in the fact that not being heard is an issue which is often raised as a point of criticism of healthcare professionals by patients and their families.
Careful observation and reports of subjective symptoms are the window through which healthcare professionals gain knowledge of their patients. Following on from the opening chapters this volume is structured to enable the healthcare professional to learn how to systematically gather information before moving on to an initial diagnosis and further investigations. The tools of inspection, palpation, percussion, and auscultation are key to this assessment and excellently laid out in the chapters covering the examination of the different organs of the body, different age groups, and some specialist topics. Professor Cox has also helpfully included in the appendix a number of the widely used standardised instruments to assess such areas as disability, activities of daily living, reading, and mental state.
It is key for healthcare professionals to be able to communicate the outcomes of their Physical Assessment to their professional colleagues. In the final chapter Professor Cox demonstrates her experience and understanding of the world of healthcare when she talks about the importance of this communication between professionals and how the Physical Assessment can bring together disparate professional views which will underpin the diagnostic process.
Professor Cox is a consummate professional who has been an educator for most of her career with a focus on clinical practice and the patient experience. She couples her educational activity with an extensive research record on nursing practice. In Physical Assessment for Nurses and Healthcare Professionals, Professor Cox has created an invaluable guide that will not only support practitioners as they enter into a clinical career in healthcare but which can be used as an ongoing reference book to support their careers as they move into advanced practice.
Professor Stanton Newman
Preface
Over the past two to three decades, many changes have been seen in the roles of healthcare professionals. Significant changes have been seen in the allied health professions, nursing, and midwifery. It is common practice now to see the healthcare professional functioning as an independent practitioner with specialist/advanced practice qualifications. For example, to list but a few, it is not uncommon to find audiologists, nurses, midwives occupational therapists, opticians, physiotherapists, and radiotherapists with master's and doctoral degrees diagnosing and treating patients. These practitioners are expected to know how to provide expert holistic health‐oriented care for culturally diverse populations. Specialist/advanced practice health professionals view the patient as an individual with physical as well as emotional, psychological, intellectual, social, cultural, and spiritual needs. A comprehensive assessment of the patient is the foundation upon which healthcare decisions are made. The best way to develop assessment skills is to learn them systematically. The systematic approach involves taking a full health history, conducting a physical examination, and reviewing diagnostic tests/laboratory data. Use of advanced assessment skills are essential in clinical decision making that leads to the formulation of a differential diagnosis and final diagnosis.
This text for healthcare professionals is based on Turner and Blackwood's Lecture Notes on Clinical Skills that was written for medical students. It is intended to be used as a reference book that can be reviewed near the patient in the clinical setting. In general, the pages are arranged with simple instructions on the left, with important aspects requiring action marked with a bullet (•). Subsidiary lists are marked with a dash (–). On the right are brief details of clinical situations and diseases that are relevant to abnormal findings. In this edition, colour photographs of assessment techniques have been added as well as case studies to assist healthcare practitioners in their assessment of the patient.
Turner and Blackwood's Lecture Notes on Clinical Skills has been used in the Oxford Clinical Medical School for over 40 years and is viewed as an essential guide for medical students globally. It should be noted that although some doctors may use slightly different techniques in taking a history and physical examination, it is recommended that healthcare practitioners embarking on a career as specialist/advanced practitioners use the techniques recommended in this text because they provide a sound approach for developing and employing clinical decision making.
Carol Lynn Cox, PhD, RN
Acknowledgements
Special thanks are extended to Robert Turner and Roger Blackwood for granting permission for their text, Lecture Notes on Clinical Skills, to be revised as a text originally for nurses. I am grateful to my students for encouraging me to revise the original text so that they could have an accessible resource for reference purposes in the clinical setting. The Turner and Blackwood text still serves as a reference for the third edition which has been expanded for all healthcare practitioners. Sincere gratitude is expressed to Sandra Kerka for thoroughly reviewing this book and correcting a multitude of errors therein and to Vincent Rajan, Production Editor, for efficiently bringing the book to completion. Finally, I am grateful to the Health and Hope Clinics of Pensacola Florida; City University, London, England; and the University of Latvia, Department of Optometry and Vision Science, Latvia, for supporting this project through their generous provision of physical assessment technique photographs. Any faults or omissions in this book are entirely my own.
Figures appearing on pp. 36, 37, 41, 49 (Figure 3.1), 52 (Figure 3.2), 53 (Figure 3.3), 54, 55 (Figure 3.4), 56 (Figure 3.5), 69 (Figure 3.11), 75 (Figures 4.1 and 4.2), 76 (Figure 4.3), 77 (Figures 4.4 and 4.5), 78 (Figure 4.6), 81 (Figure 4.7), 82 (Figure 4.9) and 83 (Figure 4.10) are reproduced with permission of City University from Advanced Practice: Physical Assessment (1997), Carol Lynn Cox, Professor, City University London, St Bartholomew School of Nursing and Midwifery, ISBN 1900804255, Reprinted 2002.
The visual acuity reading charts (Appendices A and B) are reproduced courtesy of Keeler Ltd.
Introduction: The First Approach
Carol Lynn Cox
General Principles
It is important to understand that for the purposes of examination, assessment, and diagnosis, doctors are framing their approach to the patient from the perspective of the medical model. However, you must recognise that as an allied healthcare practitioner, you are employing the medical model within your frame of practice. Therefore, to be wholistic, the approach incorporates all aspects of your particular discipline (e.g. audiology, nursing, midwifery, physiotherapy, occupational therapy, radiography, respiratory therapy, speech therapy).
General Objectives
When you approach a patient there are four initial objectives you should consider:
Obtain a professional rapport with the patient and gain their confidence.
Obtain all relevant information that allows assessment of the illness and provisional diagnoses.
Obtain general information regarding the patient and their background, social situation, and problems. In particular, it is necessary to find out how the illness has affected the patient, their family, friends, colleagues, and life.
A wholistic assessment of the patient is of utmost importance.
Understand the patient's own ideas about their problems, major concerns, and expectations of the hospital admission, outpatient, or general practice consultation.
Remember medicine is just as much about worry as disease. Whatever the illness, whether chest infection or cancer, anxiety about what may happen is often uppermost in the patient's mind (Clark 1999; Japp and Robertson 2013; NHS Wales 2010).
Listen Attentively (Engage in Active Listening.)
Engage in active listening
The following notes provide a guide as to how the healthcare practitioner obtains the necessary information.
Specific Objectives
In taking a history or conducting a physical examination there are several complementary aims:
Obtain all possible information about a patient and the illness (a database) from both a subjective and objective perspective.
Consider all possible differential diagnoses related to the patient and the illness.
Formulate the diagnoses from the patient's subjective, objective physical examination and investigative tests (e.g. laboratory, radiologic, and other).
Solve the problem as to the diagnoses (Bickley and Szilagyi
2013
; Japp and Robertson
2013
; Jarvis
2015
).
Analytical Approach
For each symptom or sign you need to think of a differential diagnosis and of other relevant information (from the history, physical examination, and/or investigative tests) that will be needed to support or refute possible diagnoses. A good history, physical examination, and investigation include these two facets and can be viewed as either positive (support) or negative (refute) findings. To achieve a formal diagnosis, following differential diagnosis, critical thinking/clinical decision making is used to examine positive and negative findings. Healthcare practitioners frequently find that using the first two components of the Subjective, Objective, Assessment, and Plan (SOAP) (Clark 1999) format can help them formulate their diagnosis. You should never approach the patient with just a set series of rote questions. Frequently in preassessment clinics, ambulatory services (outpatient) clinics, or general practice settings, standard assessment forms within an electronic patient record (EPR) are used as a guide to history taking. However, there are some instances in which paper records are employed. These tools provide the necessary basis for a later, more inquisitive approach that should develop as knowledge about the patient's problem is acquired. Key to the process of achieving a diagnosis and formulating a plan of care is listening carefully to the patient, taking time, not assuming a diagnosis when the patient initially expresses their chief complaint, and understanding your own values, attitudes, and beliefs as they relate to diverse patient populations (Japp and Robertson 2013).
Focus on the patient
The ‘subjective’ and objective components of the SOAP format provide a basis for diagnosis. Within the subjective component, the patient's perspective of the problem/illness is stated in their own words. This is often listed as the patient's chief complaint. In addition, the patient's ‘subjective’ view of their health history (e.g. childhood diseases and immunisations) as well as family history, present medications, how and when the patient takes the medications, and chronological ordering of sequelae leading to the presenting problem are documented. The objective component consists of your physical examination and investigative tests. Assessment involves the formulation of a diagnosis from the history, physical examination, and investigative tests. Plan involves the development of the plan of care for the patient as well as where, when, how, and by whom the plan will be implemented (Bickley and Szilagyi 2013).
Self‐Reliance – Getting Started
You must take your own history, make your own examination, and write your own clinical records. After a month or two you should be sufficiently proficient that your notes can become part of the final medical record. You should add a summary including your assessment of the problem list, provisional diagnoses, and preliminary investigations. Initially when developing your assessment/examination skills these will be incomplete and occasionally incorrect. Nevertheless, the exercise will help to inculcate an enquiring approach and to highlight areas in which further questioning, investigation, or study/reading is needed.
What Is Important When You Start?
At the basis of all practice is clinical competence. No amount of knowledge will make up for poor technique.
Over the first few weeks it is essential to learn the basics of history taking and physical examination. This involves:
how to relate to patients
how to take a good history efficiently, knowing which question to ask next and avoiding leading questions
how to examine patients in a logical manner, in a set routine that will mean you will not miss an unexpected sign
You will be surprised how often healthcare practitioners can fail an exam, not because of lack of knowledge but because they have not mastered elementary clinical skills. These notes are written to try and help you to identify what is important and to help relate findings to common clinical situations.
There is nothing inherently difficult about history taking and physical examination. You will quickly become clinically competent if you:
apply yourself
initially learn the skills that are appropriate for each situation
Common Sense
Common sense is the cornerstone of good practice.
Always be aware of the patient's needs.
Always evaluate what important information is needed:
to obtain the diagnosis
to provide appropriate treatment
to ensure continuity of care at home.
Many mistakes are made by being sidetracked by aspects that are not important. Remain focused on the patient.
Learning
Your clinical skills and knowledge can soon develop with good organisation.
Take advantage of seeing as many patients
in acute care (hospital and ambulatory clinics) and in primary care (the community) as possible. It is particularly helpful to be present when patients are being admitted as emergencies or are being seen in an ambulatory clinic or general practice setting for the first time.
Obtain a wide experience of clinical diseases
, how they affect patients, and how they are managed.
The more patients you can clerk yourself, the sooner you will become proficient and the more you will learn about patients and their diseases.
Building Up Knowledge
At first history taking and physical assessment seem like a huge subject and each fact you learn seems to be an isolated piece of information. How will you ever be able to learn what is required? You will find after a few months that the information related to each system interrelates with other systems. The pieces of the jigsaw puzzle begin to fit together and then your confidence will increase. Although you will need to learn many facts, it is equally important to acquire the attitude of questioning, reasoning, and knowing when and where to go to seek additional information.
Choose a medium‐sized textbook in which you can read about each disease you see or each problem you encounter.
Attaching knowledge to individual patients is a great help in acquiring and remembering facts. To practice history taking and physical assessment/examination without a textbook is like a sailor without a chart, whereas to study books rather than patients is like a sailor who does not go to sea.
Understand the scientific background of disease, including the advances that are being made and how these could be applied to improve care. (The world wide web is a good resource as well as scientific journals for gaining knowledge that will assist you in building your knowledge.)
Regularly read the editorials or any articles that interest you in scientific journals.
Even if at first you are not able to put information into context, they will keep you in touch with new developments that add interest. Nevertheless, it is not sensible to delve too deeply into any one subject when you are just beginning.
Relationships
Good relationships with patients and clinical colleagues are essential. You should maintain a natural, sincere, receptive, and supportive relationship with your patients and clinical colleagues. Your ultimate goal in working with patients and clinical colleagues is to achieve good care (Department of Health, Social Services and Public Safety in Northern Ireland 2016; Jarvis 2015).
Your Role as an Advanced Healthcare Practitioner
Your role as an advanced healthcare practitioner extends the boundaries of the scope of professional practice. The skills and practices associated with advanced practice involve using advanced clinical assessment techniques, interpreting diagnostic tests including diagnostic imaging, implementing and monitoring therapeutic regimes, prescribing pharmacological interventions, initiating and receiving appropriate referrals, and discharging patients (NMC 2005; HCPC 2013a, b; HCPC 2016).
Practice associated with the advanced practice role in healthcare involves:
Assessment and management of patient illness/health status
The healthcare practitioner–patient relationship
Prescribing medicines, ordering diagnostic investigations and treatments
An education function – including undertaking continuing education
The professional role of the healthcare practitioner
Managing and negotiating healthcare delivery systems
Monitoring and ensuring quality of advanced healthcare practice
Respecting culture and diversity (HCPC
2013a
,
b
,
2016
; NHS Wales
2010
; RCN
2002
,
2008
,
2012
; RCN Scotland
2015
).
It is essential that you develop sound skills within the framework delineated here if you expect to be competent at the specialist/advanced practice level.
References
Bickley, L. and Szilagyi, P. (2013).
Bates' Guide to Physical Examination and History Taking
, 11e. New York: Wolters Kluwer/Lippincott Williams & Wilkins.
Clark, C. (1999). Taking a history. In:
Nurse Practitioners, Clinical Skills and Professional Issues
(ed. M. Walsh, A. Crumbie and S. Reveley). Oxford: Butterworth Heinemann.
Department of Health, Social Services and Public Safety in Northern Ireland (2016).
Advanced Nursing Practice Framework: Supporting Advanced Nursing Practice in Health and Social Care Trusts
. Belfast: NIPEC.
HCPC (2013a).
Standards of Proficiency
. London: Health & Care Professions Council.
HCPC (2013b).
Standards of Prescribing
. London: Health & Care Professions Council.
HCPC (2016).
Standards of Conduct, Performance and Ethics
. London: Health & Care Professions Council.
Japp, A. and Robertson, C. (2013).
Macleod's Clinical Diagnosis
. Edinburgh: Churchill Livingstone, Elsevier.
Jarvis, C. (2015).
Physical Examination and Health Assessment
, 7e. Edinburgh: Elsevier.
NHS Wales (2010).
Framework for Advanced Nursing, Midwifery and Allied Health Professional Practice in Wales
. Llanharan: National Leadership and Innovation Agency for Healthcare.
NMC (2005). Annex 1 domains of practice and competencies. In:
NMC Consultation on a Proposed Framework for Post‐Registration Nursing
. London: Nursing and Midwifery Council.
RCN (2002).
Advanced Nurse Practitioners – An RCN Guide to the Nurse Practitioner Role, Competencies and Programme Accreditation
. London: Royal College of Nursing.
RCN (2008).
Advanced Nurse Practitioners – An RCN Guide to the Advanced Nurse Practitioner Role, Competencies and Programme Accreditation
. London: Royal College of Nursing.
RCN (2012).
Advanced Nurse Practitioners – An RCN Guide to the Advanced Nurse Practitioner Role, Competencies and Programme Accreditation
. London: Royal College of Nursing.
RCN Scotland (2015).
Nurse Innovators: Clinical Decision‐Making in Action
. Edinburgh: Royal College of Nursing.
Chapter 1Interviewing and History Taking
Carol Lynn Cox
General Procedures
Introduction
The patient's history is the major subjective source of data about their health status. Physiological, psychological, and psychosocial information (including family relationships and cultural influences) can be obtained which will inform you about the patient's perception of current health status and lifestyle. It will give you insight into actual and potential problems as well as providing a guide for the physical examination. History taking involves obtaining the patient's chief complaint, a full review of systems from the patient's perspective, exploration of patient problems associated with the chief complaint, and other (frequently associated) problems that require addressing from the patient's perspective (Ball et al. 2014a, b; Barkauskas et al. 2002; Bickley and Szilagyi 2007, 2013; Cox 2010; Dains et al. 2012, 2015; Epstein et al. 2008; Japp and Robertson 2013; Jarvis 2008, 2015; Seidel et al. 2006, 2010; Swartz 2006; Talley and O'Connor 2006, 2014).
Ensure your patient is seated comfortably for the interview
Approaching the Patient
Put the patient at ease by being confident and quietly friendly (Hatton and Blackwood
2003
; Jackson and Vessey
2010
; Rudolf and Levene
2011
; Sawyer
2012
).
Greet the patient: ‘Good morning, Mr/Mrs Smith’. (Address the patient formally and use the full name until the patient has given you permission for less formal address.)
Shake the patient's hand or place your hand on theirs if the patient is ill. (This action begins your physical assessment. It will give you a baseline indication of the patient's physical condition. For example, cold, clammy, diaphoretic, or pyrexial.)
State your name and title/role.
Make sure the patient is comfortable.
Explain that you wish to ask the patient questions to find out what happened.
Start the history taking by stating something like ‘I will start the history by asking you some questions about your health’. (Always begin with general questions and then move to more specific questions (Cox
2010
) Inform the patient how long you are likely to take and what to expect. For example, after discussing what has happened to the patient, explain that you would like to examine them.
Usual Sequence of Events
Figure 1.1 depicts the sequence of events in an examination.
Figure 1.1 Usual sequence of events.
Importance of the History
It identifies:
what has happened
the personality of the patient
how the illness has affected the patient and family
any specific anxieties
the physical and social environment.
It establishes the practitioner–patient relationship.
It provides the foundation for your differential diagnoses.
It often gives the diagnosis.
Find the principal symptoms or symptom. Ask one of the following questions:
‘How may I help you?’
‘What has the problem been?’
‘Tell me why have you come to the surgery/clinic/hospital today?’ or ‘Tell me why you came to see me today?’
Effective history taking involves allowing the patient to talk in an unstructured way whilst you maintain control of the interview. Use language that the patient can understand and avoid the use of medical jargon (Collins‐Bride and Saxe
2013
; Cox
2010
; Sawyer
2012
; Tally and O'Connor
2014
). Avoid asking questions that can be answered by a simple ‘yes’ or ‘no’. Ask questions that require a graded response. For example, ‘Describe how your headache feels.’ Avoid using multiple‐choice questions that may confuse the patient (Cox
2010
; Jackson and Vessey
2010
). Ask one question at a time. Avoid asking questions like: ‘What's wrong?’ or ‘What brought you here?’ Use clarification to confirm your understanding of the patient's problem. Avoid forming premature conclusions about the patient's problem and above all remain nonjudgemental in your demeanour. Avoid making judgemental statements.
Let the patient tell their story in their own words as much as possible.
At first listen and then take discreet notes as the patient talks.
When learning to take a history there can be a tendency to ask too many questions in the first two minutes. After asking the first question you should normally allow the patient to talk uninterrupted for up to two minutes.
Do not worry if the story is not entirely clear or if you do not think the information being given is of diagnostic significance. If you interrupt too early, you run the risk of overlooking an important symptom or anxiety.
You will be learning about what the patient thinks is important. You have the opportunity to judge how you are going to proceed. Different patients give histories in very different ways. Some patients will need to be encouraged to enlarge on their answers to your questions; with other patients, you may need to ask specific questions and to interrupt in order to prevent too rambling a history. Think consciously about the approach you will adopt. If you need to interrupt the patient, do so clearly and decisively. Most important, do not give the impression you are in a hurry to conclude the discussion as this impression may cause the patient to withhold valuable information you need before commencing your physical examination.
Try, if feasible, to conduct a conversation rather than an interrogation, following the patient's train of thoughts.
You will usually need to ask follow‐up questions on the main symptoms to obtain a full understanding of what they were and of the chain of events.
Obtain a full description of the patient's principal complaints.
Enquire about the sequence of symptoms and events.
Beware pseudomedical terms, e.g. ‘gastric flu’ – enquire what happened. Clarify by asking what the patient means.
Do not ask leading questions.
A central aim in taking the history is to understand patients' symptoms from their own point of view. It is important not to tarnish the patient's history by your own expectations. For example, do not ask a patient whom you suspect might be thyrotoxic: ‘Do you find hot weather uncomfortable?’ This invites the answer ‘yes’ and then a positive answer becomes of little diagnostic value. Ask the open question: ‘Do you particularly dislike either hot or cold weather?’ (Ball et al.
2014a
,
b
; Bickley and Szilagyi
2013
; Coulehan
2006
).
Be sensitive to a patient's mood and nonverbal responses.
For example, hesitancy in revealing emotional content. Use reflection so that the patient will expand on their discussion.
Be understanding, receptive, and matter of fact without being sympathetic. Display and express empathy rather than sympathy.
Avoid showing surprise or reproach.
Clarify symptoms and obtain a problem list.
When the patient has finished describing the symptom or symptoms:
briefly summarise the symptoms
ask whether there are any other main problems (Coulehan
2006
)
For example, say, ‘You have mentioned two problems: pain on the left side of your tummy, and loose motions over the last six weeks. Before we talk about those in more detail, are there any other problems I should know about?’
Usual Sequence of History
nature of principal complaints, e.g. chest pain, poor home circumstances
history of present complaint
details of current illness
enquiry of other symptoms (see Functional Enquiry)
past history
family history
personal and social history
If one's initial enquiries make it apparent that one section is of more importance than usual (e.g. previous relevant illnesses or operation), then relevant enquiries can be brought forward to an earlier stage in the history (e.g. past history after finding principal complaints).
History of Present Illness
Start your written history with a single sentence summing up what your patient's complaint is. It should be like the banner headline of a newspaper. For example: c/o chest pain for six months.
(You may choose to state the patient's chief complaint in the patient's own words when documenting.)
Determine the chronology of the illness by asking:
‘How and when did your illness begin?’ or
‘When did you first notice anything wrong?’ or
‘When did you last feel completely well?’
Begin by stating when the patient was last perfectly well. Describe symptoms in chronological order of onset.
Both the date of onset and the length of time prior to being seen by you should be recorded. Symptoms should never be dated by the day of the week as this later becomes meaningless (Bickley and Szilagyi
2007
,
2013
; Cox
2010
).
Obtain a detailed description of each symptom by asking:
‘Tell me what the pain was like’, for example. Make sure you ask about all symptoms, whether they seem relevant or not.
With all symptoms obtain the following details:
duration
onset – sudden or gradual
what has happened since:
constant or periodic
frequency
getting worse or better
precipitating or relieving factors
associated symptoms.
If pain is a symptom also determine the following:
site
radiation
character, e.g. ache, pressure, shooting, stabbing, dull
severity, e.g. ‘Did it interfere with what you were doing?’ ‘Does it keep you awake?’ ‘Have you ever had this type of pain before?’ ‘Does the pain make you sweat or feel sick to your stomach?’
Avoid technical language when describing a patient's history. Do not say ‘the patient complained of melaena’, rather: ‘the patient complained of passing loose, black, tarry motions’.
Supplementary History
When patients are unable to give an adequate or reliable history, the necessary information must be obtained from friends or relations. A history from a person who has witnessed a sudden event is often helpful.
When the patient does not speak English, arrange for an interpreter to translate for the patient. Bear in mind that numerous authors (Barkauskas et al. 2002; Ball et al. 2014a; Bickley and Szilagyi 2013; Cox 2010; Jarvis 2015; Rhoads and Paterson 2013) indicate that if possible family members and patients' young children should not be used as interpreters. Family members will frequently tell you what they think the patient's problem is rather than what the patient thinks the problem is. Because some questions that you may ask the patient are sensitive in nature, children should not be asked to interpret for their parents (Cox 2010; Lack 2012).
Functional Enquiry
This is a checklist of symptoms not already discovered.
Do not ask questions already covered in establishing the principal symptoms. This list may detect other symptoms.
Modify your questioning according to the nature of the suspected disease, available time, and circumstances (Lack
2012
).
If during the functional enquiry a positive answer is obtained, full details must be elicited.
Asterisks (*) denote questions that must nearly always be asked.
General Questions (These May Be Considered as Part of Your Review of Systems.)
Ask about the following points:
*appetite: ‘What is your appetite like? Do you feel like eating?’
*weight: ‘Have you lost or gained weight recently?’
*general well‐being: ‘Do you feel well in yourself?’
*feelings of sadness or depression (to rule out feelings of suicide): ‘Do you feel sad or depressed?’
fatigue: ‘Are you more or less tired than you used to be?’
fever or chills: ‘Have you felt hot or cold? Have you shivered?’
night sweats: ‘Have you noticed any sweating at night or any other time?’
aches or pains
rash: ‘Have you had any rash recently? Does it itch?’
lumps and bumps
Cardiovascular and Respiratory System
Ask about the following points:
*chest pain: ‘Have you recently had any pain or discomfort in the chest?’
The most common causes of chest pain are:
ischaemic heart disease
: severe constricting, central chest pain radiating to the neck, jaw, and left arm;
angina
: pain frequently precipitated by exercise or emotion and relieved by rest;
myocardial infarction
; the pain may come on at rest, be more severe, and last hours
pleuritic pain
: sharp, localised pain, usually lateral; worse on inspiration or cough
anxiety or panic attacks
: a very common cause of chest pain Enquire about circumstances that bring on an attack.
*shortness of breath: ‘Are you breathless at any time?’
Breathlessness (dyspnoea) and chest pain must be accurately described. The degree of exercise that brings on the symptoms must be noted (e.g. climbing one flight of stairs, after 0.5 km [1/4 mi] walk).
shortness of breath on lying flat (
orthopnoea
): ‘Do you get breathless in bed? What do you do then? Does it get worse or better on sitting up? How many pillows do you use? Can you sleep without them?’
waking up breathless: ‘Do you wake at night with any symptoms? Do you gasp for breath? What do you do then?’
Orthopnoea (breathless when lying flat) and paroxysmal nocturnal dyspnoea (waking up breathless, relieved on sitting up) are features of left heart failure.
*
ankle swelling
Common in congestive cardiac failure (right heart failure).
palpitations: ‘Are you aware of your heart beating?’
Palpitations may be:
single thumps (
ectopics
)
slow or fast
regular or irregular
Ask the patient to tap them out.
Paroxysmal tachycardia (sudden attacks of palpitations) usually starts and finishes abruptly.
*cough: ‘Do you have a cough? Is it a dry cough or do you cough up sputum? When do you cough?’
sputum: ‘What colour is your sputum? How much do you cough up?’
Green sputum usually indicates an acute chest infection. Clear sputum daily during winter months suggests chronic bronchitis. Frothy sputum suggests left heart failure.
*blood in sputum (
haemoptysis
): ‘Have you coughed up blood?’
Haemoptysis must be taken very seriously. Causes include:
carcinoma of bronchus
pulmonary embolism
mitral stenosis
tuberculosis
bronchiectasis
blackouts (
syncope
): ‘Have you had any blackouts or faints? Did you feel light‐headed or did the room go round? Did you lose consciousness? Did you have any warning? Can you remember what happened?’
*smoking: ‘Do you smoke? How many cigarettes do you smoke each day?’
Gastrointestinal System
Ask about the following points:
nausea: ‘Are there times when you feel sick?’
vomiting: ‘Do you vomit? What is it like?’
‘Coffee grounds’ vomit suggests ‘altered’ blood such as with a bleeding ulcer.
Old food suggests pyloric stenosis.
If blood what colour is it – dark or bright red?
difficulty in swallowing (
dysphagia
): ‘Do you have difficulty swallowing? Where does it stick?’
For solids: often organic obstruction.
For fluids: often neurological or psychological.
indigestion: ‘Do you have any discomfort in your stomach after eating?’
abdominal pain: ‘Where is the pain? How is it connected to meals or opening your bowels? What relieves the pain?’
*bowel habit: ‘How often do you open your bowels?’ or ‘How many times do you open your bowels per day?’ ‘Do you have to open your bowels at night?’ (often a sign of true pathology)
If diarrhoea is suggested, the number of motions per day and their nature (blood? pus? mucus?) must be established. Frothy, frequent diarrhoea may be suggestive of coeliac disease.